On behalf of the PLTC DE&I Committee, we would like to share below the February, 2021 statement from the Asian American Psychological Association (AAPA) and Stop AAPI Hate condemning recent violence against Asian elders. Additional resources are provided.
Statement Condemning Violence Against Asian and Asian
Americans February 10, 2021
The Asian American Psychological Association (AAPA) and Stop
AAPI Hate unequivocally condemn the increasing hate and violence directed
toward Asians and Asian Americans nationwide and most recently in northern
California, which resulted in the death of one Asian American elder. We mourn
the loss of and seek justice for Vicha Ratanapakdee, one of several victims in
a string of attacks targeting Asian and Asian American seniors. As an
organization and community of immigrants, refugees, and People of Color, we are
especially distressed by these events because of the continued violence
targeting Asian Americans, as discussed in our April 2020 COVID-19
Racism-related Statement. These are not isolated incidents, and the atrocities
committed against Asians and Asian Americans intensify the challenges that our
community is already facing. The attacks on our elders are especially horrific
because it reflects an intentional targeting of the most revered and also most
vulnerable members of our community. The violence is happening at a time when
Asian Americans are already disproportionately impacted by the COVID-19
pandemic, from economic instability and unemployment to being on the front
lines as essential healthcare workers.
Preliminary findings from AAPA’s ongoing collaborative
research with the Stop AAPI Hate reporting center show that as of January 2021,
a total of 2,808 reports were received documenting a range of discrimination
and violence inflicted on the AAPI community. Thus far, 7.3% of the incidents
reported to the portal are from individuals 60 years of age and older. This is
likely an underreported percentage, but one that reveals our elders being
targets of race-based discrimination. Findings also indicated that overall,
respondents experienced hate incidents as traumatic, now perceive their country
as much more dangerous, view anti-Asian discrimination as a primary source of
stress, and are in need of more mental health support than there is available.
More findings will be forthcoming.
We stand with the 40+ Asian American and Asian immigrant
organizations in the Bay Area that convened yesterday morning to condemn the
anti-Asian violence against the AAPI community. We will work in tandem to
develop cross-cultural coalitions and healing, promote trauma-informed and
culturally-sensitive services, and build safety within and across our
communities. We encourage Asian Americans to attend to their individual and
collective mental health during this time of fear, uncertainty, anger, and
grief. We urge our community and allies to strive for unity instead of
division, and to offer solidarity in the fight against racism. This includes
intervening when possible, validating the pain of those who are distressed, and
reporting anti-Asian hate crimes, including the ones they directly experience
and those that they witness (see links below). We remind members of our
community to seek justice and support for victims without perpetrating
anti-Blackness and overpolicing as a means to restore a sense of safety. We
will not demonize or scapegoat any communities of color. We will continue to
advocate for additional education, support, and resources to invest in the
community-building and safety of all of our people.
On behalf of the PLTC DE&I Committee, Please see below a list of notable February, Holidays and Observances:
Black History Month (observed for the full month of
February):
According to History.Com
(https://www.history.com/topics/black-history/black-history-month), “Black History Month is an annual
celebration of achievements by African Americans and a time for recognizing
their central role in U.S. history. Also known as African American History
Month, the event grew out of “Negro History Week,” the brainchild of noted
historian Carter G. Woodson and other prominent African Americans. Since 1976,
every U.S. president has officially designated the month of February as Black
History Month. Other countries around the world, including Canada and the
United Kingdom, also devote a month to celebrating Black history…Since 1976, every American president has designated
February as Black History Month and endorsed a specific theme. The Black History Month 2021 theme, ‘Black
Family: Representation, Identity and Diversity’ explores the African diaspora,
and the spread of Black families across the United States.”
February 1: National Freedom Day, which
celebrates the signing of the 13th Amendment that abolished slavery in 1865.
February 3: Setsubun-Sai (Beginning of Spring),
the day before the beginning of spring in Japan, celebrated yearly as part of
the Spring Festival.
February
12: Lunar New Year is the first day of the year according to
the lunar (lunisolar) calendar. This year it falls on February 12. In many
parts of the world, people know of it as Chinese New Year. In Chinese
communities, the celebration ends on the 15th day of the new year with the
Lantern Festival. Other Asian communities all over the world also follow the
lunar calendar, so lunar new year is celebrated across cultural and ethnic
groups. It is an important time for family reunion and delicious food; a time
to reflect on the past and prepare for a bright future.
February 16: Vasant Panchami, the Hindu festival
that highlights the coming of spring. On this day Hindus worship Saraswati
Devi, the goddess of wisdom, knowledge, music, art, and culture.
February 16: Mardi Gras, Carnival, Fat Tuesday, Shrove
Tuesday: This holiday takes place on the day
before Ash Wednesday, the first day of Lent, the 40-day period that precedes
Easter. The type of celebration or name
of the holiday depends on the country of origin and local traditions.
February 17: Ash Wednesday, the first day of
Lent on the Christian calendar. Its name is derived from the symbolic use of
ashes to signify penitence.
February 20: World day of social justice. Was declared an annual celebration by the UN
General Assembly in 2007.
February 21: International Mother Language Day. This holiday has been observed every year since
February 2000 to promote linguistic and cultural diversity and
multilingualism.
February 25-28: Intercalary Days or Ayyám-i-Há,
celebrated by people of the Bahá’í faith. At this time, days are added to the
Bahá’í calendar to maintain their solar calendar. Intercalary days are observed
with gift giving, special acts of charity, and preparation for the fasting that
precedes the New Year. People of the
Bahá’í Faith also participate in a 19-day fast from Feb. 28 – March 19
to reinvigorate the soul and bring one closer to God. This fast takes place immediately before the
beginning of the Bahá’í New Year.
February 25-26: Purim, a Jewish celebration that
marks the time when the Jewish community living in Persia was saved from
genocide. On Purim, Jewish people offer charity and share food with friends.
February 27: Maghi-Purnima, a Hindu festival
especially for worshippers of Lord Vishnu. Millions of devotees take a holy
bath on this day. Devotees also carry out charity work on this day.
As we (finally!) ring in a new year and say goodbye and good riddance to 2020, we at PLTC and the PLTC Diversity, Equity and Inclusion Committee (DE&I) want to bring everyone’s attention to the 2021 Diversity Calendar – which has increased significance for understanding and celebrating diversity in the United States.
While holidays and celebrations may take many forms and may be celebrated to varying degrees, in a country as diverse as the United States, there are recognitions that are as varied as the population, from month long celebrations to more specific observances. Some are more somber remembrances or sacrifice or tragedy, while others represent achievements. Still others focus on a person, religion or heritage.
It is not possible to cover every event; however, we would like to highlight some of those events that are recognized by many. Here are some key dates for the coming month of January that focus on diverse segments we feel are worth knowing about for the work that we do with our older adult clients:
Notable January 2021 Holidays and Observances:
January 4 – World Braille Day: Held on January 4th of each year to commemorate the birthdate of Louis Braille, the inventor of braille, World Braille Day is observed in order to raise awareness of the importance of braille as a means of communication, issues of accessibility and independence, and the full realization of the human rights for blind and partially sighted people.
January 17 – World Religion Day: Every year on the third Sunday of January, people from all cultures and backgrounds come together to celebrate the commonalities of different faiths around the world, of which there are over 4,000 recognized religions. The holiday was initiated by the Baháʼí in 1950 to promote interfaith harmony and understanding, as their faith emphasizes the importance of universal equality and unity.
January 18 – Martin Luther King Day: The third Monday of January each year honors the life of American clergyman and activist Dr. Martin Luther King, Jr.. Best known for the use of nonviolent civil disobedience as a means to advance the civil rights cause, he was one of the civil rights movement’s most prominent leaders from the mid-1950s until his assassination in 1968. The date is celebrated as Civil Rights Day in some states, and commemorates Dr. King’s birth.
January 27 – International Holocaust Remembrance Day: This international day of remembrance is held each year to commemorate the memory of the over 6 million Jews and 11 million other victims of the Holocaust. It is, to quote the remarks of former president Barack Obama, a time to “mourn the loss of lives, celebrate those who saved them, honor those who survived, and contemplate the obligations of the living.” It was on January 27th in 1945 that Soviet troops liberated the Auschwitz-Birkenau concentration camp.
The COVID-19 pandemic continues to produce uncertainty, stress, and trauma in our communities. All of us who work in healthcare have been touched by this pandemic. We’ve lost people we cared for; we’ve sacrificed time with our loved ones. Many of us have gotten COVID or lost a family member to it. Despite experiencing months of unspeakable tragedy and the challenges we are all facing every day, this is also a time that is bringing out the best in many people—from the first-responders fighting on the front-lines to the essential workers providing food, products, and services. As our own wise colleague Dr. Eleanor Feldman Barbera recently reminded us: “Let us hope the losses and trials of the pandemic lead to increased recognition of our value and interconnectedness, more compassionate care for elders, and to post-traumatic growth.”
We are all in this together. In the meantime, please stay safe and healthy, and we wish you all the best for a brighter year ahead.
Transgender Awareness Week, typically taking place the second week of November, has been a one-week observation to help raise visibility about transgender people and address issues members of the community face. The week culminated in the annual November 20th Transgender Day of Remembrance, a day to honor the memory of transgender people whose lives were lost in acts of anti-transgender violence over the past year.
To further the inclusivity of
transgender older adults in mental health care, Dr. Regina Koepp, a
nationally-recognized clinical psychologist and gerontologist and creator of
the Psychology
of Aging Podcast, recently hosted Loree Cook-Daniels, M.S., a renowned expert in
transgender aging and founder of the transgender aging network, on the topic of
providing affirming care for transgender older adults.
In the episode, Cook-Daniels discussed clinical considerations for mental health providers providing treatment to transgender older adults, such as the relationship and social factors affected when someone transitions earlier in life versus later, and the disproportionately high rates of mental health concerns, suicidal thoughts, and discrimination that transgender individuals face in the healthcare system.
Cook-Daniels also notes the unique
role that mental health providers historically have played as “gatekeepers” to
determine an individual’s ability to tolerate gender-affirming hormone therapy
or surgeries. She comments on the potential consequences this role can have in
deterring some transgender people from seeking mental health care due to a
concern that the provider may deny them access to these necessary treatment or
procedures.
Finally, she shares a number of
free resources for family, friends, mental health and medical providers, and
other geriatric care providers. As each of us have an important role to creatie
safe and secure spaces for healing for transgender older adult clients, we
encourage you to check out these
resources and informative, insightful podcast episode with one of
the nation’s leading experts on this important topic.
Michael William Vincent Mackie Jr., Ph.D. On behalf of the PLTC Public Policy Committee
It has been a
difficult year for our members at PLTC, both personally and professionally. No
one anticipated the extent of the unprecedented impacts of the COVID-19
pandemic on our long-term care communities. We recognize the sacrifices
you have made this year and are so very proud of the heroic work done by our
members.
As we near the end
of 2020, we wanted to summarize for you the work done over the course of this
year by your PLTC Public Policy Committee.
We began the year
by reaching out to our members directly to better understand issues important
to you and tried our best to work towards these goals in our advocacy
opportunities throughout the year.
One of the issues
echoed by our membership was the importance of designating psychologists as physicians
to help streamline the care we could provide to our patients. This is an
ongoing struggle and the committee continues to advocate on your behalf with
our legislatures. Lisa Lind has been pivotal in reaching out and meeting
virtually with representatives Burgess and Veasey to underscore the improved
timely access to care that such a designation would have for our patients in
LTC. Throughout the year there were several meetings with the APA and the
above congressional offices to advocate for the Medicare Mental Health Access
Act (HR884). You may have seen emails from our committee members with
requests to share your stories related to delayed access to mental health care
due to issues surrounding physician orders. These individual patient
stories are extremely helpful when advocating for change and we appreciate all
who participated.
Jennifer Birdsall
was instrumental in strengthening our relationship with the different
organizations with which we work, collaborating with the APA and CMS to advocate
for these changes during crucial times of the pandemic. In May of this
year, Jennifer Birdsall spoke on behalf of psychologist, with the support of
Stephen Gillaspy, the Senior Director of Health Care Financing at APA and Doug
Walter, JD, Associate Executive Director of Practice Government Relations at
APA, to Demetrios Kouzoukas, the Principle Deputy Administrator and Director of
the center for Medicare Services on a number of advocacy topics. These
included: 1) Updating the definition of physician to include psychologists, 2)
preventing rate cuts and removing the need for budget neutrality, and 3)
continuing reimbursement for telehealth and audio-only services during the
pandemic.
Lisa Lind also
coordinated with Stephen Gillapsy, the Senior Director of Health Care Financing
and Dr. Valle Wright, the Senior Director of Health Care Innovation to help
support relevant MIPS measure and reporting capabilities in LTC. These meetings
were helpful to address the possible changes in measures used by MIPS, as well
as identifying the negative impact COVID-19 had on the reporting of these
measures. More recently, she met with Nicole Owings-Fonner, Director of
Operations of APA’s Health Care Innovation and the MBHR committee to discuss
how to make MIPS measures more relevant to our patients.
Also of great
importance to our membership was Medicare’s proposed update to the physician
fee schedule and reduction in reimbursement rates in 2021 as a result of the
E&M code revision and budget neutrality. The Public Policy
Committee, along with help from our membership, tirelessly worked to advocate
for appropriate reimbursement for psychology providers across CPT
codes.
The Public Policy
Committee is grateful to be able to serve our members and support you, as well
as others in the field of psychology, and in particular for those working with
older adults to ensure patient access to quality care. We want to thank all our
members who have helped support the many initiatives we have brought to your
attention this year. Many of you have responded to our calls to action,
which is pivotal to successful advocacy.
We want to hear
from you. Our survey this year has helped guide our committee’s
priorities, but please reach out at any time with any requests or suggestions
for how the PLTC Public Policy Committee can best serve you. Please do
not hesitate to contact our members, Lisa Lind, Jennifer Birdsall, Cecilia
Poon, or Mike Mackie, should you have any more specific questions about the
work done or future advocacy opportunities.
Wishing you and your
families a very joyful, safe, and healthy holiday season. Again, thank
you for the heroic and essential work you do, caring for our nation’s older
adults.
The PLTC Diversion, Equity, and Inclusion Committee (DE&I) announces action on the part of APA CEO Dr. Arthur C. Evans Jr. in August to call for comprehensive policy changes to end the pandemic of racism in the United States.
Joined by American Psychiatric
Association CEO Dr. Saul Levin and National Association of Social Workers CEO
Dr. Angelo McClain, the national leaders in mental health published an op-ed in
the Orlando Sentinel that addressed the systemic racism that led to the deaths
of George Floyd, Breonna Taylor, and many other Black Americans over the past
year. They also expressed concern regarding the disproportionate impact
COVID-19 has had on communities of color and commit to increase action within
their respective organizations to address racial disparities in the United
States, including the recruitment of more people of color in the mental health
profession.
Additionally, they emphasize that
the ending of systemic racism is a public health priority that requires
immediate action on the part of policymakers. Among the policy changes they
call for are:
Increased access
to healthcare for people of color, who face disproportionate barriers to
access and quality of care;
Improved
access to and elimination of restrictions on telehealth;
Police
and law enforcement reform that includes training in de-escalation
techniques, banning of the use of chokeholds, and elimination of racial
and religious profiling;
Passing
the George Floyd Justice in Policing Act (R.7120/S.3912), a bill with wide-ranging measures proposed to
increase law enforcement accountability;
Passing
the bipartisan Crisis Care Improvement and Suicide Prevention Act (R.7159) to authorize increased funds for the provision of
mental health crisis services; and
Response
to mental health crises with trained mental health professionals rather
than armed police.
To read the full text of the
article, please click here.
From time to time, communications on behalf of the DE&I
Committee may include information from other organizations or advocacy groups
in the diversity, equity, and inclusion space. We believe this information can
help spark discussions, further the exchange of ideas and best practices, and
ultimately help further PLTC’s purpose, among other goals, to provide advocacy
on ethical, regulatory, organizational, and public policy issues which impact
individuals and professionals in long-term care. It is not intended to support
or oppose any partisan political views, beliefs, or ideology.
In the wake of recent events across the USA, the PLTC Board set out to form a Diversity Committee. At this time, 7 individual PLTC members have stepped forward to form the inaugural Diversity, Equity, and Inclusion Committee. The Committee will be chaired by longtime PLTC member Dr. Julie Gersch.
Dr. Julie Gersch(DE&I Committee Chair) completed her Ph.D. in Counseling Psychology at the University of Akron, Ohio. She completed her predoctoral internship in St. Paul, Minnesota in the Career and Counseling Center at the University of St. Thomas. Throughout her career, Julie has had the opportunity to engage in strong relationships with a diverse range of professionals and clinicians, forming strong collaborative working alliances with practitioners, partner communities, and referring physicians and staff.
MEET THE REST OF THE COMMITTEE
We are pleased to welcome the following additional PLTC members to serve on this crucial committee: Cecilia Poon, Katherine Lou, Hallie Nuzum, Kate King, Jennifer Birdsall, and PLTC President, Lisa Lind. We warmly encourage any additional PLTC members who wish to contribute to our burgeoning multitude of ideas, objectives, and efforts to send an email to julieschmittgersch@yahoo.com. Committee meetings will be held bimonthly and hosted on a virtual audio/visual platform.
Hallie Nuzum, Ph.D., (pronouns: she/her) graduated with her
doctorate in clinical psychology from the University of Notre Dame. She
recently completed her internship at the VA West Los Angeles and fellowship at
the VA Palo Alto, each with an emphasis in geropsychology. She now works as a
geropsychologist in outpatient mental health at the VA Puget Sound – Seattle
Division. She is excited to serve on PLTC’s DE&I Committee to work toward
equity for older adults of all identities and cultures.
Katherine Lou, PsyD, is a geropsychologist in private
practice in Boston, MA. Prior to starting her practice, she served as a
consulting psychologist in skilled rehabilitation and nursing home settings.
She strives to affirm different forms of inclusion and diversity, such as race,
religion, gender identity, sexuality, disability, and immigration status.
Katherine King, PsyD is a clinical psychologist
specializing in geropsychology. She is an assistant professor of psychology in
the clinical psychology doctoral program at William James College and has a
small private practice. She is also on the board of the Massachusetts
Gerontology Association. Dr. King writes a blog for Psychology Today and is a
passionate advocate for the well-being of helping professionals. Learn more
about Kate at www.drkateking.com
Dr. Jennifer Birdsall is the Clinical Director of CHE Behavioral Health Services, a nationwide organization providing interdisciplinary behavioral health services to residents in long-term care facilities. She specializes in clinical geropsychology and has a licensed psychologist in the states of California, New York, and Connecticut. She has over a decade of experience working in skilled nursing facilities and emphasizes a 1) whole person centered care model, and 2) a systems-level approach to behavioral health service delivery to maximize positive outcomes. She is actively involved in professional service roles, including APA’s Society of Clinical Geropsychology, APA’s Division 20: Adult Development and Aging, Psychologists in Long-Term Care (PLTC), and CA’s Partnership to Improve Dementia Care.
Cecilia Poon, PhD, ABPP (pronouns: she/her) is a board-certified geropsychologist. She is a staff psychologist and the clinical health psychology internship training director at Nebraska Medicine. She co-chairs the internship consortium’s DEI committee; and seeks to bring people of all ages, abilities, and cultures together.
Lisa Lind, Ph.D. is the current PLTC President, and is proud to serve at the pleasure of the DE&I Committee, and believes the work this committee will be advancing is even more important than ever.
PLTC is a diverse, inclusive, and empathically minded organization. The Diversity, Equity, & Inclusion Committee is dedicated to PLTC’s core values of equity and social justice within our organization. Our work aims to serve PLTC members, our clients and patients, and the community at large.
Some of
the initiatives we seek to engage in include:
1. Develop the PLTC diversity mission statement
2. Organize a task force to create multicultural guidelines and standards for clinical services to diverse populations within the LTC setting
3. Analyze and raise the diversity, equity, and inclusivity muscle on PLTC outreach efforts such as our website, newsletter, social media, and CE offerings
4. Develop resources for members to address discrimination in LTC settings
5. Support and sponsor CEU training opportunities on diversity topics
We welcome feedback on other goals you would like the DE&I Committee to work toward and accomplish together to the benefit of our membership and the clients and communities PLTC members serve.
For this initial introduction of the DE&I Committee, we invite you to take a moment to review the important July 20, 2020 press release from the HHS Office for Civil Rights if you have not yet had the opportunity to do so. It has spurred some thoughtful reflection and meaningful exchange in our committee communications.
OCR Issues Guidance on Civil
Rights Protections Prohibiting Race, Color, and National Origin
Discrimination During COVID-19
Yesterday, the Office for Civil Rights (OCR)
at the U.S. Department of Health and Human Services (HHS) is issuing guidance
to ensure that recipients of federal financial assistance understand that they
must comply with applicable federal civil rights laws and regulations that
prohibit discrimination on the basis of race, color, and national origin in
HHS-funded programs during COVID-19. This Bulletin focuses on recipients’
compliance with Title VI of the Civil Rights Act of 1964 (Title VI).
To help ensure Title VI compliance during the
COVID-19 public health emergency, recipients of federal financial assistance,
including state and local agencies, hospitals, and other health care providers,
should:
Adopt policies to
prevent and address harassment or other unlawful discrimination on the basis of
race, color, or national origin.
Ensure – when site
selection is determined by a recipient of federal financial assistance from HHS
– that Community-Based Testing Sites and Alternate Care Sites are accessible to
racial and ethnic minority populations.
Confirm that existing
policies and procedures with respect to COVID-19 related services (including
testing) do not exclude or otherwise deny persons on the basis of race, color,
or national origin.
Ensure that
individuals from racial and ethnic minority groups are not subjected to
excessive wait times, rejected for hospital admissions, or denied access to
intensive care units compared to similarly situated non-minority individuals.
Provide – if part of
the program or services offered by the recipient – ambulance service,
non-emergency medical transportation, and home health services to all
neighborhoods within the recipient’s service area, without regard to race,
color, or national origin.
Appoint or select
individuals to participate as members of a planning or advisory body which is
an integral part of the recipient’s program, without exclusions on the basis of
race, color, or national origin.
Assign staff,
including physicians, nurses, and volunteer caregivers, without regard to race,
color, or national origin. Recipients should not honor a patient’s request for
a same-race physician, nurse, or volunteer caregiver.
Assign beds and rooms,
without regard to race, color, or national origin.
Make available to
patients, beneficiaries, and customers information on how the recipient does
not discriminate on the basis of race, color, or national origin in accordance
with applicable laws and regulations.
OCR is responsible for enforcing Title VI’s
prohibitions against race, color, and national origin discrimination. As part
of the federal response to this public health emergency, OCR will continue to
work in close coordination with our HHS partners and recipients to remove
discriminatory barriers which impede equal access to quality health care,
recognizing the high priority of COVID-19 testing and treatment.
Roger Severino, OCR Director, stated,
“HHS is committed to helping populations hardest hit by COVID-19,
including African-American, Native American, and Hispanic communities.”
Severino concluded, “This guidance reminds providers that unlawful racial
discrimination in healthcare will not be tolerated, especially during a
pandemic.
“Minorities have long experienced disparities
related to the medical and social determinants of health – all of the things
that contribute to your health and wellbeing. The COVID-19 pandemic has
magnified those disparities, but it has also given us the opportunity to
acknowledge their existence and impact, and deepen our resolve to address
them,” said Vice Admiral Jerome M. Adams, Surgeon General, MD, MPH.
“This timely guidance reinforces that goal and I look forward to working
across HHS and with our states and communities to ensure it is implemented.”
To learn more about non-discrimination on the
basis of race, color, national origin, sex, age, and disability; conscience and
religious freedom; and health information privacy laws, and to file a complaint
with OCR, please visit: www.hhs.gov/ocr.
I was greatly saddened to learn that Dr. Michael Duffy, age 77, had died from pulmonary fibrosis on May 10,2020 in Canyon Lake, Texas. Michael, proud of his Irish ancestry, was born in England, the youngest of seven children. His career was long and distinguished as a counseling psychologist who significantly advanced the field of geropsychology through his teaching, mentoring, direct care of older adults, engagement in applied research and leadership in many professional organizations, including Psychologists in Long Term Care.
Michael began his career as a Catholic priest. His early training
included the Licentiate in Theology from the Angelicum University, Rome, Italy,
followed by a Postgraduate Diploma in Psychology from University College,
Dublin, Ireland and Ph.D. in Counseling Psychology from the University of Texas
in Austin.
Dr. Duffy was Professor Emeritus at Texas A&M University
since 2011. During his 30 plus years of teaching he mentored numerous students,
many of whom have become luminaries in geropsychology in their own right such
as Bradley Karlin, Tammi Vacha-Haase and the late Royda Crose from Ball State
University, to name just a few.
Michael not only taught in the classroom, but he used the
long-term care setting as a real-life classroom in his practicum courses,
conducting rounds on patients, similar to the model commonly used in medicine
but rarely incorporated in graduate psychological training.
Other teaching roles include past Director of Training of
the doctoral program in counseling psychology at Texas A&M and past
Director of the Proficiency Program in Clinical Geropsychology.
Active in retirement, Dr. Duffy maintained his license in
Texas and Limited-Pro Bono in Florida. He was a National Register Health
Service Psychologist (USA), a Diplomate in Counseling Psychology of the
American Board of Professional Psychology (ABPP), board certified in Psychology
and a Chartered Psychologist (CPsychol) of the British Psychological Society. He had over 45 years of experience as a
psychotherapist, specializing in psychological services with older adults since
1977. In post-retirement he offered pro bono psychotherapy to priests and
trained staff in rural mental health agencies in Texas.
Dr. Duffy not only mentored graduate students but also made
a concerted effort to welcome young professionals to become involved in the
field of geropsychology while he was National Coordinator in the early 1980s of
the fledgling organization, Psychologists in Long Term Care (PLTC). I know
this first hand because shortly after I obtained my psychology license I searched
for a professional home. Due to Michael’s support, friendly collegiality and warm
encouragement, I (PHS) became active in PLTC. Michael and I worked on several
professional projects together, including the committee chaired by Peter
Lichtenberg that first developed standards of practice in long-term care over
20 years ago.
In his role as the first coordinator of PLTC, Dr. Duffy was
the model of a scientist practitioner who understood the iterative nature of
science and practice. He stressed the need for a balance in PLTC between psychologists
in academia and psychologists ‘in the field’, and encouraged training programs to
make room for both. He was a particularly
strong advocate for payment systems in LTC and other geriatric settings. He encouraged
budding geropsychology students to learn their craft and make geropsychology a
career for which trainees aspired not only because they gained great satisfaction
in helping frail older adults but also because they were remunerated according
to their expertise and years of training experience. His organization of the
annual meeting of PLTC alternately at APA[MV1]
and GSA reflected his ambitious goals, and was always attended by
representatives of APA’s Office on Aging, and by those who purveyed the latest
in research, training, business news, and advocacy. One of his main tasks for
PLTC was to publish a directory of psychologists working in long-term care categorized
by state, and which included a professional profile of each psychologist and their
contact information for ease of referral.
Held in high esteem by his peers is evidenced by the fact he
was Past President (1996) of the Texas Psychological Association (TPA);
Professor of the Year, Texas Psychological Association Division of Students in
Psychology (1998); Psychologist of the Year, Texas Psychological Association
(2005); and awarded by PLTC for his outstanding Contributions in 2009.
A Fellow of the American Psychological Association (APA,
Divisions 17 and 29), he also has held several APA appointments: Member of the
APA Committee on Aging (CONA); Vice President for Professional Practice, APA
Division of Counseling Psychology; Chair, APA Board for the Advancement of
Psychology in the Public Interest (BAPPI); and Liaison to the Division of
Counselling Psychology of the British Psychological Society, of which he is a
member, Chartered Psychologist and expatriate.
A pioneering advocate for geropsychology in numerous educational
and practitioner-oriented venues, Dr. Duffy was founder and chair of the first
Texas Consortium of Educators in Gerontology, served as Medicare Committee
Chair for the Texas Psychological Association and Commissioner on the APA’s Recognition
of Specialties and Proficiencies in Professional Psychology, to name just a few
ways he made a visible and important difference in the field.
Michael was a prolific writer, reviewer and editor. He contributed
to several noteworthy landmark initiatives including the first APA guidelines
task force for psychological practice with older adults, and the launching of
the Pikes Peak conference which spawned the Pikes Peak model for training in
professional geropsychology. In these roles, Dr. Duffy helped identify the
attitudes, knowledge, and skills necessary for one to be considered a competent
geropsychologist. These conceptual developments directly led to geropsychology being
admitted as a specialty by the Council of Recognition of Specialties and
Proficiencies in Professional Psychology, thereby serving as a springboard for
geropsychology to become a specialty board of ABPP and allowing the credentialing
of individual geropsychologists.
His research included the study of intergenerational family
relations, geriatric crisis management, mental health in long term care;
religious dimensions of psychotherapy; developmental psychotherapy; and
personality styles of psychotherapists. He also developed a paraprofessional
training program for providing volunteer mental health services in nursing
homes (Project OASIS). One of the authors of this article (VM) was a psychologist
at the Houston Veterans Affairs Medical Center where Dr. Duffy promoted Project
Oasis and is struck by how prescient his thinking was regarding the use of
trained volunteers in the frequently resource-starved contract nursing homes
where Veterans who needed long term care were placed years ago (prior to the development
of the CLCs).
Dr. Powell Lawton, one of the founders of the field of professional
geropsychology, was a mentor to Michael and was very supportive of his research
on the psychological effects of nursing home design shared an interest in
environmental psychology with Dr. Duffy. They both studied the psychological
impact of building design and how ‘disruptive’ behavior of those with dementia
can be viewed as failures of design rather than necessarily intrinsic to the
nature of dementia. In addition to publishing many peer- reviewed journal
articles and book chapters, in 1999 he edited one of the first handbooks of
counseling and psychotherapy with older adults that remains relevant today.
Clearly Dr. Duffy has not only contributed to but also helped
to shaped the field of geropsychology by his tireless groundbreaking and
pioneering work. Dr. Duffy practiced what he preached and taught, did research,
developed a private practice, and advocated at the state and local levels for
geropsychology. He will be sadly missed by his many colleagues and friends and his
immediate family members, wife Jo Ann and three children, Sara Michelle, Claire
Marie who is a psychologist, and Andrew Justin.
From our personal encounters with Michael over 35 years, we will remember his unique combination of a gentle, peaceful countenance, generosity, political acumen, deep spirituality and wry British wit.
PLTC continues to be at the forefront of advocating for it’s members! Last week, PLTC President Lisa Lind wrote a letter to CMS administrator Seema Verma on the subject of the recent telehealth waiver (which we discussed in our previous post, below).
There’s a lot Dr. Lind’s letter (text below, at the end of the post), and a lot that’s been going on with COVID-19 and mental health services provision in long-term care that go even beyond telehealth.
For one thing, on the PLTC listserv, many of our members have reported that they have been unable to gain entrance to their facilities since the COVID-19 outbreak. This is concerning on a couple of different levels – for one thing, CMS has traditionally regarded psychologists as “essential personnel” who would be exempted from any ban on outside visitors or staff. Second, obviously, COVID-19 has created significant mental health stressors on our residents (due to anxiety, increased isolation, etc.) that are not going away anytime soon. So, we are asking CMS and Administrator Verma to clarify what has already been codified – that long-term care psychologists are “essential” personnel and need to be allowed to see our residents!
Second, as we noted in our last post – regarding the recent telehealth waiver (or Waiver 1137) – President Lisa Lind also asks in her letter for CMS to relax enforcement of the audiovisual requirement for telehealth. It’s difficult enough for our largely cognitively and functionally impaired population to navigate telehealth, but to require it to be only delivered via “video chat” makes this even more difficult a hurdle. If our providers are forced to rely on telehealth to see our residents because of COVID-19 – we need the flexibility to simply give them a phone call!
Please read the letter, and understand that PLTC is advocating tirelessly for our members, and for psychologists in long-term care at large. This is a challenging time for us as providers, and our clients in particular.
As always – if you have anything to share about COVID-19 or how practice with older adults is changing in the face of this pandemic, please comment on this article below.
If you are a psychologist who practices in long-term care, or work with older adults in your practice and would like to learn more, we have an active Listserv, Newsletter, and other resources. Please consider joining PLTC!
Re: COVID19 and the Importance of Allowing Mental Health Providers to Continue to Provide Medically Necessary Psychological Services to Residents in Long-Term Care Facilities During This Time of Restricted Visitation
Dear Administrator Verma:
Psychologists In Long Term Care, Inc. (PLTC) is a national organization of several hundred psychologists who contribute to improving the mental health of older adults through practice, research, education, and advocacy. Our organization represents psychologists across the nation who serve the mental health needs of older adults, particularly Medicare and Medicaid beneficiaries in need of long-term care services. As such, we are in a strong position to speak to the mental health needs of the residents of long-term care facilities.
On March 9, 2020 the Centers for Medicare & Medicaid Services (CMS) issued to State Survey Agency Directors revised guidance for Infection Control and Prevention of Corona Disease 2019 (COVID19) in nursing homes (Ref: QSO-20-14-HN). On the same day, the American Health Care Association (AHCA) and the National Center for Assisted Living (NCAL) issued a joint statement entitled “Taking Reasonable Efforts to Prevent COVID-19 from Entering Your Skilled Nursing Center”. Various state healthcare associations and Departments of Public Health have also issued similar guidance. On March 13, 2020 the Guidance for Infection Control and Prevention of Coronavirus Disease 2019 (COVID-19) in Nursing Homes included revised guidance for visitation, which indicates that “facilities should restrict visitation of all visitors and non-essential health care personnel, except for certain compassionate care situations, such as an end-of-life situation” but suggested that individuals should be able to enter if they meet the CDC guidelines for health care workers.
CMS and AHCA guidance include the recommendation to limit visitors to nursing facilities. AHCA specifically stipulates that essential healthcare providers should not be considered visitors and should not be restricted from entering facilities unless screening processes trigger concerns. Psychologists are considered as essential healthcare providers by CMS and therefore should be allowed access to nursing facilities in order to treat patients residing in long term care facilities. In addition, AHCA has indicated that facility contractors and consultants who are needed to assure the residents’ needs are met should be allowed entry. However, as an immediate result of published recommendations and subsequent media coverage, psychologists and other mental health providers have experienced a wide variety of responses from nursing facilities in response to COVID19 precautions. To help mitigate the risk of exposing nursing home residents to possible exposure to COVID19, some nursing facilities have implemented reduced visitation, restricted all visitation, and/or restricted facility staff to only essential staff members. Many facilities across the country are interpreting the guide to restrict visitors to include the restriction of mental health providers. As you may know, a large number of nursing home residents have a mental health diagnosis, and the current media coverage of COVID-19 combined with mandatory decreased in-person visits from family are contributing to observed increased anxiety in residents. Individuals with a history of trauma, even if the trauma is completely unrelated to the current situation, can be triggered in circumstances like this. In order to provide essential behavioral health services to meet the needs of nursing home residents, mental health professions will need to be able to have consistent and reliable access to entry into nursing home facilities.
I am reaching out to you, on behalf of psychologists across the United States, to request consideration of acknowledgement for the need for mental health professionals to be allowed access into nursing homes and not be considered “visitors”, rather essential healthcare workers, during the COVID19 pandemic. If this message is communicated from a government official in an esteemed position such as yours, I am optimistic that nursing homes across the country will feel more confident in allowing mental health clinical providers to continue to provide consistent mental health care to Medicare and Medicaid beneficiaries without interruption, particularly at a time when stress and anxiety is high.
In addition, many psychologists across the country have begun investigating the potential use of telehealth services in the event that it becomes increasingly difficult to provide in-person services to their patients. However, many clinicians report difficulty understanding the possible exceptions to previous rules and regulations, and when they reach out to their local MACs they are either receiving mixed information and/or being told that the new guidelines have not been communicated to them yet. As we await Secretary Azar to exercise his authority to grant the Emergency Telehealth Waiver, we look forward to additional CMS guidelines to confirm that telehealth services will no longer be limited to Medicare beneficiaries located in a designated rural health professional shortage area; and Medicare beneficiaries will not have to go to a designated “originating site” in order to receive telehealth services. This way, we can assure that beneficiaries in all nursing facilities will be eligible for telehealth services.
One potential concerning issue is the continued device requirement for “both audio and video capability”. Having the requirement for video capability will be a serious obstacle for many psychologists who want to continue to provide psychological services without interruption. Not every resident in nursing facilities has access to a smartphone. A requirement for audio and video capability would require ordering equipment and training nursing home staff to facilitate the process. Given the current circumstances, nursing facilities will continue to experience staff shortages as staff either test positive and/or have to self-quarantine due to possibly being exposed, and it will become extremely difficult for nursing homes to be able to have staff who could assist with facilitation of telehealth services if the usual equipment is required. I would ask that you consider waiving the requirement for video capability and consider allowing the use of both smart phones and traditional telephones for services during this unprecedented health crisis in order to allow for continuation of care to assist those Medicare beneficiaries who are likely experiencing increased anxiety and other mental health symptoms during this time of uncertainty. It is prudent for us to remove potential barriers to accessing mental health care in order to minimize potential increases in mental health conditions as a result of current stressors.
Finally, we believe additional directives to the telehealth waiver will also significantly improve the provision of telehealth to Medicare beneficiaries:
1) We support waiving the current requirement that providers be licensed in the State in which a patient is located, as long as they are holding an equivalent license in another State.
2) We support a directive that the waiver applies to all Medicare beneficiaries needing medical and mental health services, not only beneficiaries seeking counseling or treatment related to COVID-19. Thank you in advance for your time and consideration.
Sincerely,
Lisa Lind, Ph.D. PLTC President Psychologists In Long Term Care, Inc. llindphd@outlook.com
Image source: Norwood (Charity). Open license (CC 2.0).
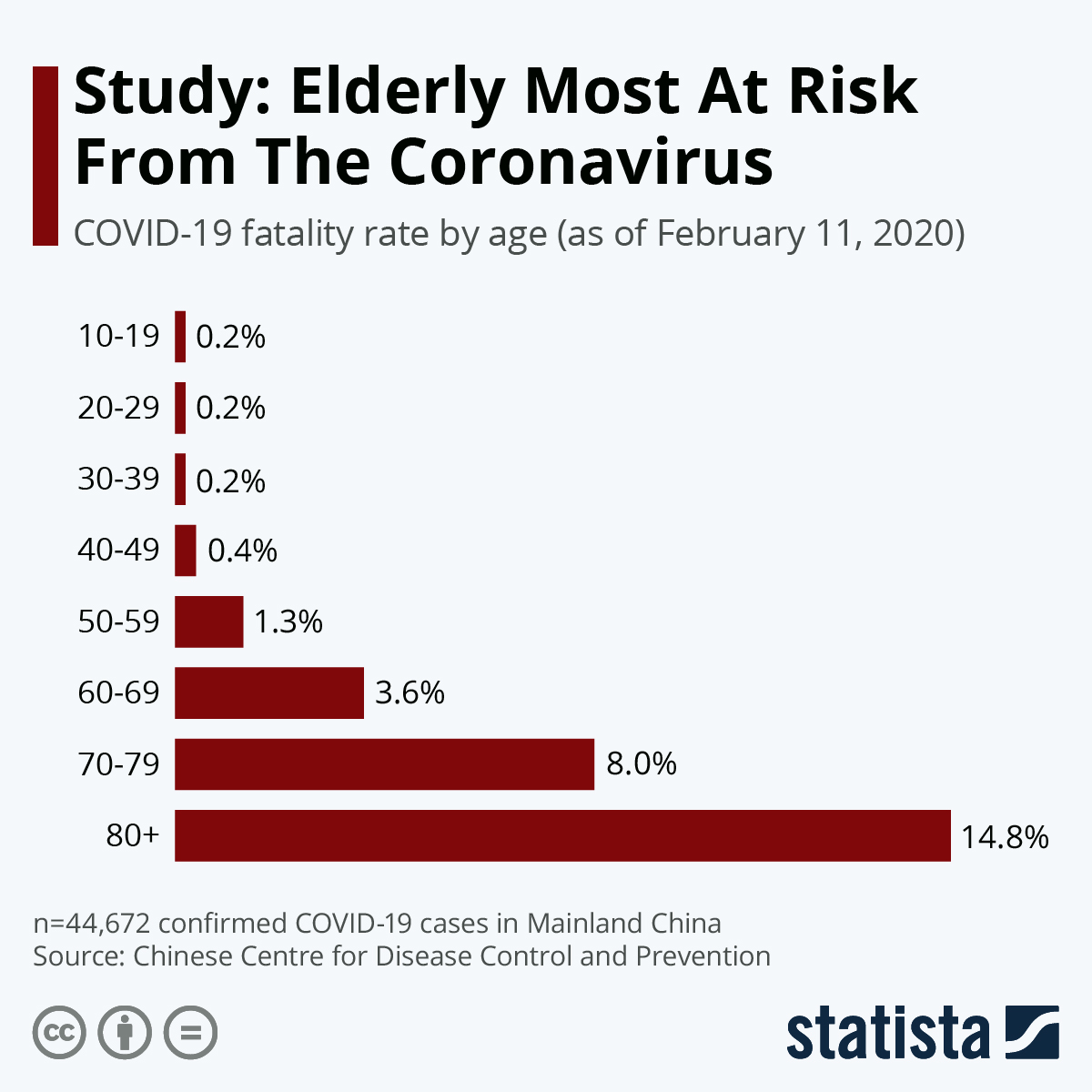
So, a viral pandemic has happened – the United States, along with the rest of the world, has had to take extreme measures to prevent the spread of a potentially deadly pathogen within our population. As it happens, this virus, also known as COVID-19, is particularly deadly to older adults and those with chronic medical conditions:
In response to this elevated threat to the older adult population, it’s now become the accepted advice that older adults should practice the most extreme forms of social distancing possible – with the US Federal Government’s Centers for Disease Control advising early on that older adults should “stay home as much as possible” and across the pond, in the UK, over-70s (all over-70s) will be subject to a mandatory quarantine for at least 4 months.
Image source: Pixabay (free to use, no license required).
For us at Psychologists in Long-Term Care, this has highlighted something we have all known for quite some time – that older adults have, up until now only limited options for seeking mental health care when they are homebound and isolated. You would think that telehealth and telemedicine would have long been able to successfully fill the gap here – but not so fast. While older adults are quickly becoming tech-savvy and comfortable with technology, regulatory and bureaucratic limitations have held things back.
In my
own personal blog and in a previous PLTC article by our esteemed former
PLTC Treasurer, Alan Duretz in our Winter/Spring 2017 Newsletter (“CMS and
Telehealth Reimbursement”), it’s been noted that while Medicare has in theory
reimbursed psychological service providers for their services (psychotherapy,
primarily) that are delivered via remote technology (so-called “e-therapy,”) in
practice the regulations and limitations placed on these services have been so
exacting that few, if any, providers have ever taken advantage of them. The
main barriers have been the following:
Requirement
that e-therapy providers need use HIPAA compliant technology with “asynchronous
store and forward” capabilities.
Requirement
that e-therapy is conducted in an audiovisual modality – e.g., telephone-only
services don’t count.
Requires
that e-therapy consumers need to be located in an HPSA, or federally-designated
Health Professional Shortage area
Requires
that e-therapy consumers receive services at an “eligible originating site”
(e.g., typically a clinic or similar healthcare facility
Requires
that e-therapy services be provided to patients with whom you have a
preexisting doctor-patient relationship (e.g., can only be provided to patients
whom you have filed Medicare claims for over the last three years).
Something extremely noteworthy and groundbreaking is
happening in the geropsychology and long-term care space in the midst of the
COVID-19 crisis. Recently,
at a press conference in Washington DC, Medicare administrator Seema Varna,
flanked by President Donald Trump, Vice President Pence, and several other
high-ranking officials, announced that they are relaxing #1, #3 #4, and #5
above (we’ll come back to #2 in a second).
In other words, this means that now, as long as
psychologists make a “good faith” attempt to safeguard the privacy of their
patients, they can now use platforms like Skype or Facetime to see older adult
patients, and not be concerned about violating the HIPAA Privacy lsw. . There
is a useful FAQ that was just released by CMS (Centers for Medicare Services)
that you can read here.
Moreover, these can be for newly-referred patients and residents in need, and
therapy can be delivered in residents homes (whether the home is a facility or
otherwise).
There’s a couple of catches, though. The waiver, known as “1135,” does not waive the requirement that providers use audiovisual modality with their patients. So, for the time being, telephone therapy is still not covered (except possibly in Texas or other states, see here). Which is unfortunate, because there are still any number of older adults out there who remain uncomfortable with videoconferencing and/or have visual limitations. Another is that the new waiver doesn’t spell out where providers can practice, so it’s not completely clear whether it’s acceptable for providers to deliver services from home, their office, or what have you (apparently APA has reached out to CMS to clarify this, and is awaiting a response).
So far, though, this is good – and really needed as the country tries to work through the COVID-19 crisis. But to me and others in PLTC – if rules and restrictions like these are to be relaxed during a crisis, it’s reasonable to ask whether these rules were necessary in the first place. COVID-19 will pass, but the problem of older adults being isolated and functionally impaired and unable to easily attend in-person medical or mental health appointments will remain, and technology is available to address these problems. Think about that.
Also, if you have anything to share about COVID-19 or how practice with older adults is changing in the face of this pandemic, please comment on this article below.
Finally, if you are a psychologist who practices in long-term care, or work with older adults in your practice and would like to learn more, we have an active Listserv, Newsletter, and other resources. Please consider joining PLTC: